


Phase III breakdown: Motixafortide versus Mozobil
a cross-trial comparison points to a new standard of care

I’ve seen a few negative reactions to the GENESIS data based on flawed cross-trial comparisons, and I’d like to dispel these misconceptions with a brief analysis.
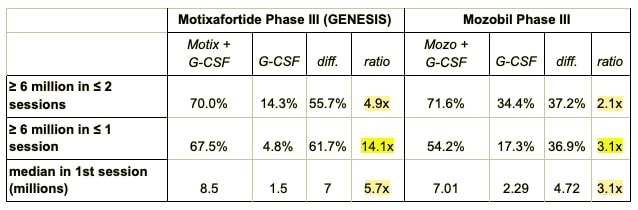
Here are the key data points from the two trials:
Absolute comparisons show disappointing results (flawed logic)
I’ve seen a number of people making absolute comparisons between the endpoint percentages for the treatment groups of the motixafortide (motix) and the Mozobil/plerixafor (mozo) phase III trials.
If we do that for the primary endpoint, for instance (≥ 6 million cells in ≤ 2 sessions), we see that motix had a 70.0% success rate, compared with a 71.6% success rate for mozo.
So mozo is the winner, right? Everyone should sell their BLRX shares and run for the hills?
Nope. Far from it.
Relative comparisons show outstanding results (sound logic)
Because the characteristics of trial populations can differ widely, we need to find the differences in outcomes between treatments and controls in each trial, then compare those differences.
In the table you will see the absolute differences between treatment and control groups for each endpoint, and next over, ratios (i.e., magnitude of improvement). Ratios are appropriate here because they are inherently relative. They show us, as clearly as possible using available data, just how good these drugs are at doing their job, compared with placebo (i.e., G-CSF alone). This allows for a rough comparison across trials.
Looking at the ratios, we see that motix outperformed mozo across the board, at least doubling relative efficacy. And just look at the percentage of patients reaching 6 million cells in 1 apheresis. It shows that motix + G-CSF resulted in a 14.1-fold improvement over G-CSF alone, compared with just 3.1-fold for mozo.
Those are excellent results!
That’s good enough for standard of care, even before considering all the savings (in time and money) that come with a single-dose regimen. (The upcoming pharmacoeconomic analysis is going to highlight this all-important aspect.)
These trials are more than a decade — and a paradigm shift — apart
Now you might be wondering why the efficacy rates in the control arms were so dramatically different between trials.
Just look at the control group success rates after the first apheresis session: The motix trial had an abysmal rate of 4.8%, compared with 17.3% in the mozo trial.
This means approximately 4 times as many patients in the mozo trial hit the mark with G-CSF alone, suggesting that the mozo trial population had far better mobilizers than the motix trial. This explains why those primary endpoint percentages, in absolute terms, are similar—because motix was fighting an uphill battle while mozo was already standing on the hill.
But wait, weren’t the inclusion/exclusion criteria the same? Shouldn’t these populations be similar?
They should be. But the finest enrollment criteria can’t unwind the hands of time.
Here’s the thing: There’s been a major paradigm shift in myeloma treatment since the mozo trial was conducted more than a decade ago. Back then, a fair number of patients were still receiving chemo as a frontline treatment, and doublet regimens were only gaining a foothold. In general, a stem cell transplant was considered earlier in the treatment sequence.
These days, myeloma patients receive continuous therapy, typically with a triplet combination, until they have disease progression, then they may have a second or even third therapy, before transplant is considered.
This means that patients are now more heavily pre-treated before they undergo transplant. And some of these new treatments may reduce their ability to mobilize.
Here’s an excerpt from a letter to the editor in Nature, which describes this issue:
There is limited data in the literature on the potential impact of daratumumab [a new therapy] on stem cell mobilization and post transplant outcomes, in patients receiving the drug prior to autologous stem cell transplant (ASCT). In the Cassiopeia trial, patients who received daratumumab in combination with bortezomib, thalidomide, and dexamethasone required more plerixafor and had a lower median number of collected and infused stem cells, compared to patients who did not receive daratumumab.
In addition to the potential for worse mobilization due to previous regimens, increased drug efficacy means that patients these days, on average, have had myeloma for longer before they receive a transplant.
I believe these two factors (impact of prior therapies and longer disease duration) largely explain the wide disparities in control rates. With relative comparisons, however, we can see that the clear frontrunner here is motixafortide.
But wait...what about new data?
I’ve seen a couple people citing high mobilization rates for mozo from newer, uncontrolled studies, but these comparisons are badly flawed by their lack of controls, since we can’t make any relative comparisons. Despite the clear differences in population characteristics, these two phase III trials remain our best source of information.
I’m a doctor and a medical journalist (often covering oncology). Yes, I’m long BLRX. No, this isn’t financial advice.
Clear and informativr